Bunions All The Things You Need To Learn
Overview
 Bunions are a common problem that most individuals experience as a painful swelling or a bony protuberance at the inner base of the big toe. This condition is the result of a malalignment of the first toe. These can be hereditary or secondary to wearing high-heeled or narrow toe-box shoes.
Bunions are a common problem that most individuals experience as a painful swelling or a bony protuberance at the inner base of the big toe. This condition is the result of a malalignment of the first toe. These can be hereditary or secondary to wearing high-heeled or narrow toe-box shoes.
Causes
Bunions are most widely considered to be due to an imbalance in the forces that is exerted across the joint during walking. The resulting abnormal motion and pressure over the joint, over many years (combined with poor fitting footwear) leads to instability in the joint causing hallux valgus and bunions. Bunions are really only a symptom of faulty foot mechanics and are usually caused by a combination of the way we walk, the foot we inherit and inappropriate footwear use.
Symptoms
Many people do not experience symptoms in the early stages of bunion formation. Symptoms are often most noticeable when the bunion gets worse and with certain types of footwear. These include shoes that crowd the toes and/or high-heeled shoes. When symptoms do occur, they may include physical discomfort or pain. A burning feeling. Redness and swelling. Possible numbness. Difficulty walking.
Diagnosis
A thorough medical history and physical exam by a physician is necessary for the proper diagnosis of bunions and other foot conditions. X-rays can help confirm the diagnosis by showing the bone displacement, joint swelling, and, in some cases, the overgrowth of bone that characterizes bunions. Doctors also will consider the possibility that the joint pain is caused by or complicated by Arthritis, which causes destruction of the cartilage of the joint. Gout, which causes the accumulation of uric acid crystals in the joint. Tiny fractures of a bone in the foot or stress fractures. Infection. Your doctor may order additional tests to rule out these possibilities.
Non Surgical Treatment
The first step in the treatment of Bunions, Corns, and Calluses is determining what is causing the problem. Check with your family doctor or Podiatrist (foot doctor) to find the best solution for your ailment. You can reduce the risk of Bunions, Corns, and Calluses by following these simple instructions. Wear properly-fitting footwear, socks, and stockings (not too tight or too loose). Wear footwear with a wide toe box (toe area). Wear footwear or arch supports which provide proper support, weight distribution, and shock absorption. Maintain a healthy weight. For early-stage Bunions, soaking your feet in warm water can provide temporary relief. 
Surgical Treatment
According to the NHS, 85 per cent of operations are successful, but there?s no guarantee that the problem won?t recur, that the pain will go away, or that your movement won?t become limited. Ask yourself if the affront to your vanity and discomfort caused by your bunion is worth the post-op suffering, and if you can cope with the inevitable restriction on your movement that means no driving and time off work, even if only for a few weeks.
Do I Suffer Over-Pronation Of The Foot
Overview
Overpronation represents a dysfunction in the biomechanics of the body, and it is not a disease. Occasionally it may make your feet ache, but it need not be that much of a problem. If you wear comfortable shoes for overpronation such as stability shoes or motion control shoes for running, that is all that is needed in most cases to prevent foot problems from developing. If you overpronate to a high degree, you may need orthopaedic devices for your shoes which will ensure the maximum amount of correction.
Causes
Unless there is a severe, acute injury, overpronation develops as a gradual biomechanical distortion. Several factors contribute to developing overpronation, including tibialis posterior weakness, ligament weakness, excess weight, pes planus (flat foot), genu valgum (knock knees), subtalar eversion, or other biomechanical distortions in the foot or ankle. Tibialis posterior weakness is one of the primary factors leading to overpronation. Pronation primarily is controlled by the architecture of the foot and eccentric activation of the tibialis posterior. If the tibialis posterior is weak, the muscle cannot adequately slow the natural pronation cycle.
Symptoms
When standing, your heels lean inward. When standing, one or both of your knee caps turn inward. Conditions such as a flat feet or bunions may occur. You develop knee pain when you are active or involved in athletics. The knee pain slowly goes away when you rest. You abnormally wear out the soles and heels of your shoes very quickly.
Diagnosis
One of the easiest ways to determine if you overpronate is to look at the bottom of your shoes. Overpronation causes disproportionate wear on the inner side of the shoe. Another way to tell if you might overpronate is to have someone look at the back of your legs and feet, while you are standing. The Achilles tendon runs from the calf muscle to the heel bone, and is visible at the back of the ankle. Normally it runs in a straight line down to the heel. An indication of overpronation is if the tendon is angled to the outside of the foot, and the bone on the inner ankle appears to be more prominent than the outer anklebone. There might also be a bulge visible on the inside of the foot when standing normally. A third home diagnostic test is called the ?wet test?. Wet your foot and stand on a surface that will show an imprint, such as construction paper, or a sidewalk. You overpronate if the imprint shows a complete impression of your foot (as opposed to there being a space where your arch did not touch the ground).
Non Surgical Treatment
Overpronation of the feet can be corrected in some cases and in others it can be effectively managed. Overpronators can train themselves to change their running gait, wear arch supports, orthotic insoles or specialist shoes for overpronators. In order to determine exactly what is happening during the stride, it is necessary to have a gait analysis conducted by a professional. The extent of overpronation can then be determined, and the causes can be identified and corrected directly. The main corrective methods used for excessive pronation are orthotics. Orthotics are the most straightforward and simplest solution to overpronation. Orthotics are devices which can be slipped into shoes which will offer varying degrees of correction to the motion of the foot. Orthotics help to support the arches and distribute the body weight effectively, and are usually the best treatment choice for moderate to severe overpronation. Orthotics may require existing insoles to be removed from your shoes to accommodate them; although most running shoes will have a removable insole to accommodate an orthotic insole.
Prevention
Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push:
Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
Overpronation represents a dysfunction in the biomechanics of the body, and it is not a disease. Occasionally it may make your feet ache, but it need not be that much of a problem. If you wear comfortable shoes for overpronation such as stability shoes or motion control shoes for running, that is all that is needed in most cases to prevent foot problems from developing. If you overpronate to a high degree, you may need orthopaedic devices for your shoes which will ensure the maximum amount of correction.
Causes
Unless there is a severe, acute injury, overpronation develops as a gradual biomechanical distortion. Several factors contribute to developing overpronation, including tibialis posterior weakness, ligament weakness, excess weight, pes planus (flat foot), genu valgum (knock knees), subtalar eversion, or other biomechanical distortions in the foot or ankle. Tibialis posterior weakness is one of the primary factors leading to overpronation. Pronation primarily is controlled by the architecture of the foot and eccentric activation of the tibialis posterior. If the tibialis posterior is weak, the muscle cannot adequately slow the natural pronation cycle.
Symptoms
When standing, your heels lean inward. When standing, one or both of your knee caps turn inward. Conditions such as a flat feet or bunions may occur. You develop knee pain when you are active or involved in athletics. The knee pain slowly goes away when you rest. You abnormally wear out the soles and heels of your shoes very quickly.
Diagnosis
One of the easiest ways to determine if you overpronate is to look at the bottom of your shoes. Overpronation causes disproportionate wear on the inner side of the shoe. Another way to tell if you might overpronate is to have someone look at the back of your legs and feet, while you are standing. The Achilles tendon runs from the calf muscle to the heel bone, and is visible at the back of the ankle. Normally it runs in a straight line down to the heel. An indication of overpronation is if the tendon is angled to the outside of the foot, and the bone on the inner ankle appears to be more prominent than the outer anklebone. There might also be a bulge visible on the inside of the foot when standing normally. A third home diagnostic test is called the ?wet test?. Wet your foot and stand on a surface that will show an imprint, such as construction paper, or a sidewalk. You overpronate if the imprint shows a complete impression of your foot (as opposed to there being a space where your arch did not touch the ground).
Non Surgical Treatment
Overpronation of the feet can be corrected in some cases and in others it can be effectively managed. Overpronators can train themselves to change their running gait, wear arch supports, orthotic insoles or specialist shoes for overpronators. In order to determine exactly what is happening during the stride, it is necessary to have a gait analysis conducted by a professional. The extent of overpronation can then be determined, and the causes can be identified and corrected directly. The main corrective methods used for excessive pronation are orthotics. Orthotics are the most straightforward and simplest solution to overpronation. Orthotics are devices which can be slipped into shoes which will offer varying degrees of correction to the motion of the foot. Orthotics help to support the arches and distribute the body weight effectively, and are usually the best treatment choice for moderate to severe overpronation. Orthotics may require existing insoles to be removed from your shoes to accommodate them; although most running shoes will have a removable insole to accommodate an orthotic insole.
Prevention
Exercises to strengthen and stretch supporting muscles will help to keep the bones in proper alignment. Duck stance: Stand with your heels together and feet turned out. Tighten the buttock muscles, slightly tilt your pelvis forwards and try to rotate your legs outwards. You should feel your arches rising while you do this exercise. Calf stretch: Stand facing a wall and place hands on it for support. Lean forwards until stretch is felt in the calves. Hold for 30 seconds. Bend at knees and hold for a further 30 seconds. Repeat 5 times. Golf ball: While drawing your toes upwards towards your shins, roll a golf ball under the foot between 30 and 60 seconds. If you find a painful point, keep rolling the ball on that spot for 10 seconds. Big toe push:
Stand with your ankles in a neutral position (without rolling the foot inwards). Push down with your big toe but do not let the ankle roll inwards or the arch collapse. Hold for 5 seconds. Repeat 10 times. Build up to longer times and fewer repetitions. Ankle strengthener: Place a ball between your foot and a wall. Sitting down and keeping your toes pointed upwards, press the outside of the foot against the ball, as though pushing it into the wall. Hold for 5 seconds and repeat 10 times. Arch strengthener: Stand on one foot on the floor. The movements needed to remain balanced will strengthen the arch. When you are able to balance for 30 seconds, start doing this exercise using a wobble board.
What Is Calcaneal Apophysitis?
Overview
Sever?s disease is the most common cause of heel pain in the growing athlete and is due to overuse and repetitive microtrauma of growth plates in the heel. It occurs in children ages 7 to 15, with the majority of patients presenting between 10 and 14 years of age. Sever?s disease will go away on its own when it is used less or when the bone is through growing, but it can recur (for example, at the start of a new sports season). Traditionally, the only known cure was for children to outgrow the condition, with recurrences happening an average of 18 months before this occurs.
Causes
Sever's disease can result from standing too long, which puts constant pressure on the heel. Poor-fitting shoes can contribute to the condition by not providing enough support or padding for the feet or by rubbing against the back of the heel. Although Sever's disease can occur in any child, these conditions increase the chances of it happening. Pronated foot (a foot that rolls in at the ankle when walking), which causes tightness and twisting of the Achilles tendon, thus increasing its pull on the heel's growth plate, flat or high arch, which affects the angle of the heel within the foot, causing tightness and shortening of the Achilles tendon, short leg syndrome (one leg is shorter than the other), which causes the foot on the short leg to bend downward to reach the ground, pulling on the Achilles tendon, overweight or obesity, which puts weight-related pressure on the growth plate
Symptoms
As a parent, you may notice your child limping while walking or running awkwardly. If you ask them to rise onto their tip toes, their heel pain usually increases. Heel pain can be felt in one or both heels in Sever's disease.
Diagnosis
X-rays are normal in Sever's disease, but your doctor will probably get X-rays to rule out other problems. Treatment consists of non-steroidal anti-inflammatory medications and use of a heel lift to relieve tension on the calcaneal apophysis. In more severe cases, phycical therapy consisting of modalities to relieve the pain, and stretching exercises may be helpful. In extreme cases, castings have been used.
Non Surgical Treatment
The practitioner should inform the patient and the patient?s parents that this is not a dangerous disorder and that it will resolve spontaneously as the patient matures (16-18 years old). Treatment depends on the severity of the child?s symptoms. The condition is self-limiting, thus the patient?s activity level should be limited only by pain. Treatment is quite varied. Relative Rest/ Modified rest or cessation of sports. Cryotherapy. Stretching Triceps Surae and strengthen extensors. Nighttime dorsiflexion splints (often used for plantar fasciitis, relieve the symptoms and help to maintain flexibility). Plantar fascial stretching. Gentle mobilizations to the subtalar joint and forefoot area. Heel lifts, Orthoses (all types, heel cups, heel foam), padding for shock absorption or strapping of heel to decrease impact shock. Electrical stimulation in the form of Russian stimulation sine wave modulated at 2500 Hz with a 12 second on time and an 8 second off time with a 3 second ramp. Advise to wear supportive shoes. Ultrasound, nonsteroidal anti-inflammatory drugs. Casting (2-4 weeks) or Crutches (sever cases). Corticosteroid injections are not recommended. Ketoprofen Gel as an addition to treatment. Symptoms usually resolve in a few weeks to 2 months after therapy is initiated. In order to prevent calcaneal apophysitis when returning to sports (after successful treatment and full recovery), icing and stretching after activity are most indicated. Respectable opinion and poorly conducted retrospective case series make up the majority of evidence on this condition. The level of evidence for most of what we purport to know about Sever?s disease is at such a level that prospective, well-designed studies are a necessity to allow any confidence in describing this condition and its treatment.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position, If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Sever?s disease is the most common cause of heel pain in the growing athlete and is due to overuse and repetitive microtrauma of growth plates in the heel. It occurs in children ages 7 to 15, with the majority of patients presenting between 10 and 14 years of age. Sever?s disease will go away on its own when it is used less or when the bone is through growing, but it can recur (for example, at the start of a new sports season). Traditionally, the only known cure was for children to outgrow the condition, with recurrences happening an average of 18 months before this occurs.
Causes
Sever's disease can result from standing too long, which puts constant pressure on the heel. Poor-fitting shoes can contribute to the condition by not providing enough support or padding for the feet or by rubbing against the back of the heel. Although Sever's disease can occur in any child, these conditions increase the chances of it happening. Pronated foot (a foot that rolls in at the ankle when walking), which causes tightness and twisting of the Achilles tendon, thus increasing its pull on the heel's growth plate, flat or high arch, which affects the angle of the heel within the foot, causing tightness and shortening of the Achilles tendon, short leg syndrome (one leg is shorter than the other), which causes the foot on the short leg to bend downward to reach the ground, pulling on the Achilles tendon, overweight or obesity, which puts weight-related pressure on the growth plate
Symptoms
As a parent, you may notice your child limping while walking or running awkwardly. If you ask them to rise onto their tip toes, their heel pain usually increases. Heel pain can be felt in one or both heels in Sever's disease.
Diagnosis
X-rays are normal in Sever's disease, but your doctor will probably get X-rays to rule out other problems. Treatment consists of non-steroidal anti-inflammatory medications and use of a heel lift to relieve tension on the calcaneal apophysis. In more severe cases, phycical therapy consisting of modalities to relieve the pain, and stretching exercises may be helpful. In extreme cases, castings have been used.
Non Surgical Treatment
The practitioner should inform the patient and the patient?s parents that this is not a dangerous disorder and that it will resolve spontaneously as the patient matures (16-18 years old). Treatment depends on the severity of the child?s symptoms. The condition is self-limiting, thus the patient?s activity level should be limited only by pain. Treatment is quite varied. Relative Rest/ Modified rest or cessation of sports. Cryotherapy. Stretching Triceps Surae and strengthen extensors. Nighttime dorsiflexion splints (often used for plantar fasciitis, relieve the symptoms and help to maintain flexibility). Plantar fascial stretching. Gentle mobilizations to the subtalar joint and forefoot area. Heel lifts, Orthoses (all types, heel cups, heel foam), padding for shock absorption or strapping of heel to decrease impact shock. Electrical stimulation in the form of Russian stimulation sine wave modulated at 2500 Hz with a 12 second on time and an 8 second off time with a 3 second ramp. Advise to wear supportive shoes. Ultrasound, nonsteroidal anti-inflammatory drugs. Casting (2-4 weeks) or Crutches (sever cases). Corticosteroid injections are not recommended. Ketoprofen Gel as an addition to treatment. Symptoms usually resolve in a few weeks to 2 months after therapy is initiated. In order to prevent calcaneal apophysitis when returning to sports (after successful treatment and full recovery), icing and stretching after activity are most indicated. Respectable opinion and poorly conducted retrospective case series make up the majority of evidence on this condition. The level of evidence for most of what we purport to know about Sever?s disease is at such a level that prospective, well-designed studies are a necessity to allow any confidence in describing this condition and its treatment.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position, If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
Achilles Tendon Rupture Treatment And Complications A Systematic Review
Overview
 An Achilles tendon rupture, also known as an Achilles tendon tear, is the snapping or pulling apart of the Achilles tendon into two pieces. Achilles tendon ruptures can be full ruptures or partial ruptures. A physician may be required to distinguish between acute Achilles tendinosis and a partial Achilles tendon rupture. Tennis Leg is a rupture of the connection between the calf muscle and the Achilles tendon. Achilles tendonitis is an inflammation of the Achilles tendon: it is much less common than, but often confused with, Achilles tendinosis. Achilles tendons can also be lacerated or crushed.
An Achilles tendon rupture, also known as an Achilles tendon tear, is the snapping or pulling apart of the Achilles tendon into two pieces. Achilles tendon ruptures can be full ruptures or partial ruptures. A physician may be required to distinguish between acute Achilles tendinosis and a partial Achilles tendon rupture. Tennis Leg is a rupture of the connection between the calf muscle and the Achilles tendon. Achilles tendonitis is an inflammation of the Achilles tendon: it is much less common than, but often confused with, Achilles tendinosis. Achilles tendons can also be lacerated or crushed.
Causes
An Achilles tendon injury might be caused by several factors. Overuse. Stepping up your level of physical activity too quickly. Wearing high heels, which increases the stress on the tendon. Problems with the feet, an Achilles tendon injury can result from flat feet, also known as fallen arches or overpronation. In this condition, the impact of a step causes the arch of your foot to collapse, stretching the muscles and tendons. Muscles or tendons in the leg that are too tight. Achilles tendon injuries are common in people who participate in the following sports. Running. Gymnastics. Dance. Football. Baseball. Softball. Basketball. Tennis. Volleyball. You are more likely to tear an Achilles tendon when you start moving suddenly. For instance, a sprinter might get one at the start of a race. The abrupt tensing of the muscle can be too much for the tendon to handle. Men older than age 30 are particularly prone to Achilles tendon injuries.
Symptoms
You may notice the symptoms come on suddenly during a sporting activity or injury. You might hear a snap or feel a sudden sharp pain when the tendon is torn. The sharp pain usually settles quickly, although there may be some aching at the back of the lower leg. After the injury, the usual symptoms are as follows. A flat-footed type of walk. You can walk and bear weight, but cannot push off the ground properly on the side where the tendon is ruptured. Inability to stand on tiptoe. If the tendon is completely torn, you may feel a gap just above the back of the heel. However, if there is bruising then the swelling may disguise the gap. If you suspect an Achilles tendon rupture, it is best to see a doctor urgently, because the tendon heals better if treated sooner rather than later.
Diagnosis
A staggering 20%-30% of Achilles tendon ruptures are missed. Thompson (calf squeeze) test is 96% sensitive and 93% sensitive. Unfortunately, some health practitioners fail to perform this simple clinical test. Ultrasound examination or an MRI can confirm an Achilles tendon rupture.
Non Surgical Treatment
Treatment for a ruptured Achilles tendon often depends on your age, activity level and the severity of your injury. In general, younger and more active people often choose surgery to repair a completely ruptured Achilles tendon, while older people are more likely to opt for nonsurgical treatment. Recent studies, however, have shown fairly equal effectiveness of both operative and nonoperative management. Nonsurgical treatment. This approach typically involves wearing a cast or walking boot with wedges to elevate your heel, which allows your torn tendon to heal. This method avoids the risks associated with surgery, such as infection. However, the likelihood of re-rupture may be higher with a nonsurgical approach, and recovery can take longer. If re-rupture occurs, surgical repair may be more difficult. 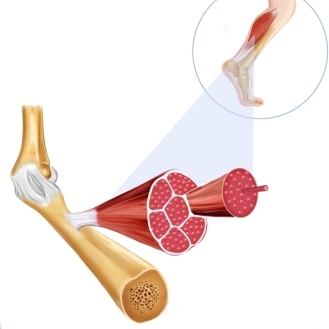
Surgical Treatment
In general, for complete tear of the tendon, surgery is recommended. For partial tears, nonsurgical treatment is recommended. However, the selection of treatment depends on the patient, age, level of activity, and other risk factors. Surgery for Achilles tendon rupture is now routine and well established. Surgery is generally suggested for the young, healthy and active individuals. For athletes, surgery is often the first choice of treatment. The Achilles tendon can be repaired surgically by either a closed or open technique. With the open technique, an incision is made to allow for better visualization and approximation of the tendon. With the closed technique, the surgeon makes several small skin incisions through which the tendon is repaired. Irrespective of type of treatment, a short leg cast (plaster) is applied on the operated ankle after completion of the procedure. The advantages of a surgical approach includes a decreased risk of re-rupture rate (0%-5%) the majority of individuals can return to their original sporting activities (within a short time), and most regain their strength and endurance. Disadvantages of a surgical approach include hospital admission, wound complications (for example, skin sloughing, infection, sinus tract formation, sural nerve injury), higher costs, and hospital admission.
Prevention
There are things you can do to help prevent an Achilles tendon injury. You should try the following. Cut down on uphill running. Wear shoes with good support that fit well. Always increase the intensity of your physical activity slowly. Stop exercising if you feel pain or tightness in the back of your calf or heel.
Leg Length Discrepancy Tests
Overview
Leg length discrepancy is a condition where the length of one leg is different than the other (shorter or longer) because of either or both a functional (muscle/posture) or structural (bone/cartilage) abnormality. In the specific a functional leg length occurs when your legs are the same, but another condition such as pelvic tilt or piriformis shortening creates the appearance of one leg being longer or shorter than the other. A structural leg length inequality it means that there is a true difference. Osteopaths, chiropractors and physiotherapist should be able to determine the degree of leg length inequality using visual inspection and manual tests.
Causes
There are many causes of leg length discrepancy. Structural inequality is due to interference of normal bone growth of the lower extremity, which can occur from trauma or infection in a child. Functional inequality has many causes, including Poliomyelitis or other paralytic deformities can retard bone growth in children. Contracture of the Iliotibial band. Scoliosis or curvature of the spine. Fixed pelvic obliquity. Abduction or flexion contraction of the hip. Flexion contractures or other deformities of the knee. Foot deformities.
Symptoms
The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result.
Diagnosis
Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement.
Non Surgical Treatment
Internal heel lifts: Putting a simple heel lift inside the shoe or onto a foot orthotic has the advantage of being transferable to many pairs of shoes. It is also aesthetically more pleasing as the lift remains hidden from view. However, there is a limit as to how high the lift can be before affecting shoe fit. Dress shoes will usually only accommodate small lifts (1/8"1/4") before the heel starts to piston out of the shoe. Sneakers and workboots may allow higher lifts, e.g., up to 1/2", before heel slippage problems arise. External heel lifts: If a lift of greater than 1/2" is required, you should consider adding to the outsole of the shoe. In this way, the shoe fit remains good. Although some patients may worry about the cosmetics of the shoe, it does ensure better overall function. Nowadays with the development of synthetic foams and crepes, such lifts do not have to be as heavy as the cork buildups of the past. External buildups are not transferable and they will wear down over time, so the patient will need to be vigilant in having them repaired. On ladies' high-heel shoes, it may be possible to lower one heel and thereby correct the imbalance.

Surgical Treatment
Your child will be given general anesthetic. We cut the bone and insert metal pins above and below the cut. A metal frame is attached to the pins to support the leg. Over weeks and months, the metal device is adjusted to gradually pull the bone apart to create space between the ends of the bones. New bone forms to fill in the space, extending the length of the bone. Once the lengthening process is completed and the bones have healed, your child will require one more short operation to remove the lengthening device. We will see your child regularly to monitor the leg and adjust the metal lengthening device. We may also refer your child to a physical therapist to ensure that he or she stays mobile and has full range of motion in the leg. Typically, it takes a month of healing for every centimeter that the leg is lengthened.
Leg length discrepancy is a condition where the length of one leg is different than the other (shorter or longer) because of either or both a functional (muscle/posture) or structural (bone/cartilage) abnormality. In the specific a functional leg length occurs when your legs are the same, but another condition such as pelvic tilt or piriformis shortening creates the appearance of one leg being longer or shorter than the other. A structural leg length inequality it means that there is a true difference. Osteopaths, chiropractors and physiotherapist should be able to determine the degree of leg length inequality using visual inspection and manual tests.
Causes
There are many causes of leg length discrepancy. Structural inequality is due to interference of normal bone growth of the lower extremity, which can occur from trauma or infection in a child. Functional inequality has many causes, including Poliomyelitis or other paralytic deformities can retard bone growth in children. Contracture of the Iliotibial band. Scoliosis or curvature of the spine. Fixed pelvic obliquity. Abduction or flexion contraction of the hip. Flexion contractures or other deformities of the knee. Foot deformities.
Symptoms
The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result.
Diagnosis
Asymmetry is a clue that a LLD is present. The center of gravity will shift to the short limb side and patients will try to compensate, displaying indications such as pelvic tilt, lumbar scoliosis, knee flexion, or unilateral foot pronation. Asking simple questions such as, "Do you favor one leg over the other?" or, "Do you find it uncomfortable to stand?" may also provide some valuable information. Performing a gait analysis will yield some clues as to how the patient compensates during ambulation. Using plantar pressure plates can indicate load pressure differences between the feet. It is helpful if the gait analysis can be video-recorded and played back in slow motion to catch the subtle aspects of movement.
Non Surgical Treatment
Internal heel lifts: Putting a simple heel lift inside the shoe or onto a foot orthotic has the advantage of being transferable to many pairs of shoes. It is also aesthetically more pleasing as the lift remains hidden from view. However, there is a limit as to how high the lift can be before affecting shoe fit. Dress shoes will usually only accommodate small lifts (1/8"1/4") before the heel starts to piston out of the shoe. Sneakers and workboots may allow higher lifts, e.g., up to 1/2", before heel slippage problems arise. External heel lifts: If a lift of greater than 1/2" is required, you should consider adding to the outsole of the shoe. In this way, the shoe fit remains good. Although some patients may worry about the cosmetics of the shoe, it does ensure better overall function. Nowadays with the development of synthetic foams and crepes, such lifts do not have to be as heavy as the cork buildups of the past. External buildups are not transferable and they will wear down over time, so the patient will need to be vigilant in having them repaired. On ladies' high-heel shoes, it may be possible to lower one heel and thereby correct the imbalance.
Surgical Treatment
Your child will be given general anesthetic. We cut the bone and insert metal pins above and below the cut. A metal frame is attached to the pins to support the leg. Over weeks and months, the metal device is adjusted to gradually pull the bone apart to create space between the ends of the bones. New bone forms to fill in the space, extending the length of the bone. Once the lengthening process is completed and the bones have healed, your child will require one more short operation to remove the lengthening device. We will see your child regularly to monitor the leg and adjust the metal lengthening device. We may also refer your child to a physical therapist to ensure that he or she stays mobile and has full range of motion in the leg. Typically, it takes a month of healing for every centimeter that the leg is lengthened.
Posterior Tibial Tendon Dysfunction Physical Therapy Exercises
Overview There's an easy way to tell if you have flat feet. Simply wet your feet, then stand on a flat, dry surface that will leave an imprint of your foot. A normal footprint has a wide band connecting the ball of the foot to the heel, with an indentation on the inner side of the foot. A foot with a high arch has a large indentation and a very narrow connecting band. Flat feet leave a nearly complete imprint, with almost no inward curve where the arch should be. Most people have "flexible flatfoot" as children; an arch is visible when the child rises up on the toes, but not when the child is standing. As you age, the tendons that attach to the bones of the foot grow stronger and tighten, forming the arch. But if injury or illness damages the tendons, the arch can "fall," creating a flatfoot. In many adults, a low arch or a flatfoot is painless and causes no problems. However, a painful flatfoot can be a sign of a congenital abnormality or an injury to the muscles and tendons of the foot. Flat feet can even contribute to low back pain.  Causes Rheumatoid arthritis This type of arthritis attacks the cartilage in the foot, leading to pain and flat feet. It is caused by auto-immune disease, where the body?s immune system attacks its own tissues. Diabetes. Having diabetes can cause nerve damage and affect the feeling in your feet and cause arch collapse. Bones can also fracture but some patients may not feel any pain due to the nerve damage. Obesity and/or hypertension (high blood pressure) This increases your risk of tendon damage and resulting flat foot. Symptoms Initially, flatfoot deformity may not present with any symptoms. However, overtime as the tendon continues to function in an abnormal position, people with fallen arches will begin to have throbbing or sharp pain along the inside of the arch. Once the tendon and soft tissue around it elongates, there is no strengthening exercises or mechanism to shorten the tendon back to a normal position. Flatfoot can also occur in one or both feet. If the arch starts to slowly collapse in one foot and not the other, posterior tibial dysfunction (PTTD) is the most likely cause. People with flatfoot may only have pain with certain activities such as running or exercise in the early phase of PTTD. Pain may start from the arch and continue towards the inside part of the foot and ankle where the tendon courses from the leg. Redness, swelling and increased warmth may also occur. Later signs of PTTD include pain on the outside of the foot from the arch collapsing and impinging other joints. Arthritic symptoms such as painful, swollen joints in the foot and ankle may occur later as well due to the increased stress on the joints from working in an abnormal position for a long period of time. Diagnosis In diagnosing flatfoot, the foot & Ankle surgeon examines the foot and observes how it looks when you stand and sit. Weight bearing x-rays are used to determine the severity of the disorder. Advanced imaging, such as magnetic resonance imaging (MRI) and computed tomography (CAT or CT) scans may be used to assess different ligaments, tendons and joint/cartilage damage. The foot & Ankle Institute has three extremity MRI?s on site at our Des Plaines, Highland Park, and Lincoln Park locations. These extremity MRI?s only take about 30 minutes for the study and only requires the patient put their foot into a painless machine avoiding the uncomfortable Claustrophobia that some MRI devices create. Non surgical Treatment Nonoperative therapy for adult-acquired flatfoot is a reasonable treatment option that is likely to be beneficial for most patients. In this article, we describe the results of a retrospective cohort study that focused on nonoperative measures, including bracing, physical therapy, and anti-inflammatory medications, used to treat adult-acquired flatfoot in 64 consecutive patients. The results revealed the incidence of successful nonsurgical treatment to be 87.5% (56 of 64 patients), over the 27-month observation period. Overall, 78.12% of the patients with adult-acquired flatfoot were obese (body mass index [BMI] = 30), and 62.5% of the patients who failed nonsurgical therapy were obese; however, logistic regression failed to show that BMI was statistically significantly associated with the outcome of treatment. The use of any form of bracing was statistically significantly associated with successful nonsurgical treatment (fully adjusted OR = 19.8621, 95% CI 1.8774 to 210.134), whereas the presence of a split-tear of the tibialis posterior on magnetic resonance image scans was statistically significantly associated with failed nonsurgical treatment (fully adjusted OR = 0.016, 95% CI 0.0011 to 0.2347). The results of this investigation indicate that a systematic nonsurgical treatment approach to the treatment of the adult-acquired flatfoot deformity can be successful in most cases.
Causes Rheumatoid arthritis This type of arthritis attacks the cartilage in the foot, leading to pain and flat feet. It is caused by auto-immune disease, where the body?s immune system attacks its own tissues. Diabetes. Having diabetes can cause nerve damage and affect the feeling in your feet and cause arch collapse. Bones can also fracture but some patients may not feel any pain due to the nerve damage. Obesity and/or hypertension (high blood pressure) This increases your risk of tendon damage and resulting flat foot. Symptoms Initially, flatfoot deformity may not present with any symptoms. However, overtime as the tendon continues to function in an abnormal position, people with fallen arches will begin to have throbbing or sharp pain along the inside of the arch. Once the tendon and soft tissue around it elongates, there is no strengthening exercises or mechanism to shorten the tendon back to a normal position. Flatfoot can also occur in one or both feet. If the arch starts to slowly collapse in one foot and not the other, posterior tibial dysfunction (PTTD) is the most likely cause. People with flatfoot may only have pain with certain activities such as running or exercise in the early phase of PTTD. Pain may start from the arch and continue towards the inside part of the foot and ankle where the tendon courses from the leg. Redness, swelling and increased warmth may also occur. Later signs of PTTD include pain on the outside of the foot from the arch collapsing and impinging other joints. Arthritic symptoms such as painful, swollen joints in the foot and ankle may occur later as well due to the increased stress on the joints from working in an abnormal position for a long period of time. Diagnosis In diagnosing flatfoot, the foot & Ankle surgeon examines the foot and observes how it looks when you stand and sit. Weight bearing x-rays are used to determine the severity of the disorder. Advanced imaging, such as magnetic resonance imaging (MRI) and computed tomography (CAT or CT) scans may be used to assess different ligaments, tendons and joint/cartilage damage. The foot & Ankle Institute has three extremity MRI?s on site at our Des Plaines, Highland Park, and Lincoln Park locations. These extremity MRI?s only take about 30 minutes for the study and only requires the patient put their foot into a painless machine avoiding the uncomfortable Claustrophobia that some MRI devices create. Non surgical Treatment Nonoperative therapy for adult-acquired flatfoot is a reasonable treatment option that is likely to be beneficial for most patients. In this article, we describe the results of a retrospective cohort study that focused on nonoperative measures, including bracing, physical therapy, and anti-inflammatory medications, used to treat adult-acquired flatfoot in 64 consecutive patients. The results revealed the incidence of successful nonsurgical treatment to be 87.5% (56 of 64 patients), over the 27-month observation period. Overall, 78.12% of the patients with adult-acquired flatfoot were obese (body mass index [BMI] = 30), and 62.5% of the patients who failed nonsurgical therapy were obese; however, logistic regression failed to show that BMI was statistically significantly associated with the outcome of treatment. The use of any form of bracing was statistically significantly associated with successful nonsurgical treatment (fully adjusted OR = 19.8621, 95% CI 1.8774 to 210.134), whereas the presence of a split-tear of the tibialis posterior on magnetic resonance image scans was statistically significantly associated with failed nonsurgical treatment (fully adjusted OR = 0.016, 95% CI 0.0011 to 0.2347). The results of this investigation indicate that a systematic nonsurgical treatment approach to the treatment of the adult-acquired flatfoot deformity can be successful in most cases.  Surgical Treatment If conservative treatments don?t work, your doctor may recommend surgery. Several procedures can be used to treat posterior tibial tendon dysfunction; often more than one procedure is performed at the same time. Your doctor will recommend a specific course of treatment based on your individual case. Surgical options include. Tenosynovectomy. In this procedure, the surgeon will clean away (debride) and remove (excise) any inflamed tissue surrounding the tendon. Osteotomy. This procedure changes the alignment of the heel bone (calcaneus). The surgeon may sometimes have to remove a portion of the bone. Tendon transfer: This procedure uses some fibers from another tendon (the flexor digitorum longus, which helps bend the toes) to repair the damaged posterior tibial tendon. Lateral column lengthening, In this procedure, the surgeon places a small wedge-shaped piece of bone into the outside of the calcaneus. This helps realign the bones and recreates the arch. Arthrodesis. This procedure welds (fuses) one or more bones together, eliminating movement in the joint. This stabilizes the hindfoot and prevents the condition from progressing further.
Surgical Treatment If conservative treatments don?t work, your doctor may recommend surgery. Several procedures can be used to treat posterior tibial tendon dysfunction; often more than one procedure is performed at the same time. Your doctor will recommend a specific course of treatment based on your individual case. Surgical options include. Tenosynovectomy. In this procedure, the surgeon will clean away (debride) and remove (excise) any inflamed tissue surrounding the tendon. Osteotomy. This procedure changes the alignment of the heel bone (calcaneus). The surgeon may sometimes have to remove a portion of the bone. Tendon transfer: This procedure uses some fibers from another tendon (the flexor digitorum longus, which helps bend the toes) to repair the damaged posterior tibial tendon. Lateral column lengthening, In this procedure, the surgeon places a small wedge-shaped piece of bone into the outside of the calcaneus. This helps realign the bones and recreates the arch. Arthrodesis. This procedure welds (fuses) one or more bones together, eliminating movement in the joint. This stabilizes the hindfoot and prevents the condition from progressing further.